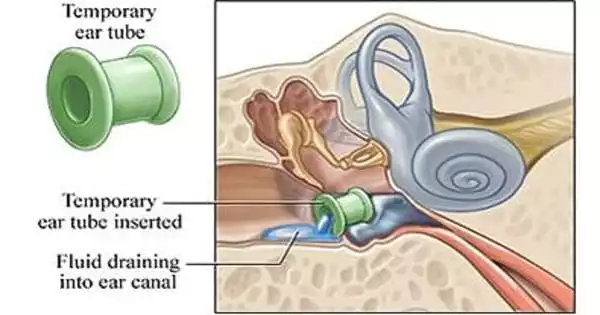
Ear infections are the most prevalent ailment in children, but they can also affect adults. Due to insufficient air exchange with the middle ear space, children are more likely to develop ear issues. The eustachian tube, a muscle tube, should be used for ear ventilation. The eustachian tube connects the middle ear to the back of the nose. Almost every child under the age of five will experience at least one ear infection (otitis media). Due to a malfunctioning eustachian tube, 15% of children will experience chronic and/or recurring ear infections.
When babies and toddlers are on a ventilator, they are at a significant risk of accumulating fluid behind their eardrum due to a tracheostomy, which is a tube surgically put into their windpipe to help relieve breathing problems. That’s the finding of a new study by UT Southwestern head and neck surgeons, published in the International Journal of Pediatric Otorhinolaryngology. This fluid buildup, known as a middle ear effusion, can put children at risk for ear infections, hearing loss, and speech and language impairments.
“The majority of the time these children are being treated, the focus is on more critical lung and heart difficulties,” said study leader Stephen R. Chorney, M.D., M.P.H., Assistant Professor of Otolaryngology — Head & Neck Surgery at UTSW and Pediatric Otolaryngologist at Children’s Health. “However, our research implies that we should also be aware of seemingly insignificant issues, such as ear effusions, because they can have an influence on communicative skills and developmental milestones in a vulnerable subset of children.”
The majority of the time these children are being treated, the focus is on more critical lung and heart difficulties. However, our research implies that we should also be aware of seemingly insignificant issues, such as ear effusions, because they can have an influence on communicative skills and developmental milestones in a vulnerable subset of children.
Stephen R. Chorney
Many young children who require tracheostomy tubes were born prematurely with undeveloped lungs or restricted airways. In some circumstances, doctors may attach a mechanical ventilator to the tracheostomy tube, which is a type of life support that helps a child breathe.
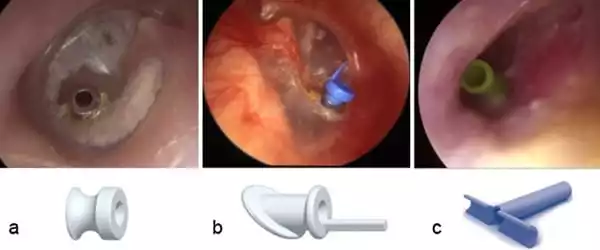
Middle ear effusion (MEE) is a common problem for all young children. Nearly one in ten kids have ear tubes placed to help clear this fluid, treat infections, and reduce hearing loss. Dr. Chorney and his colleagues suspected, based on their own observations, that tracheostomy-dependent children on a ventilator might be at a higher risk of MEE.
The new study examined 94 children at Children’s Medical Center Dallas who had a tracheostomy before the age of two between 2015 and 2020. The children, on average, had a tracheostomy at 5 months of age and then had hearing tests on a regular basis to determine the presence of MEE. In the two years following their tracheostomy, 74% of children who required mechanical ventilation acquired at least one MEE, but just 31% of those who were not on the ventilator developed one. Mechanical ventilation predicted the presence of a MEE after adjusting for age, craniofacial condition diagnosis, and newborn hearing test results. Furthermore, 80 percent of MEEs lasted for at least many months between multiple hearing assessments in all children with a tracheostomy.
“This information provides us with an objective reference point when interacting with parents,” Dr. Chorney explained. “We know this is a common occurrence, and we may consider ear tubes for some of these children.”
Because inserting ear tubes necessitates general anesthesia, certain children with tracheostomies on ventilator support may not be appropriate candidates, and the new data assists clinicians in weighing risks and advantages. Dr. Chorney would like to investigate the influence of MEEs on hearing and communication in this population in future studies.
Most children who have ventilation tubes implanted will hold the tubes in place in their eardrum for 12-18 months before being forced out of the eardrum into the ear canal. The eardrum will mend on its own, and the ear will resume normal function (i.e., dependent on its natural eustachian tube function). Children who utilize ventilation tubes to treat their ear infections are at a low risk (5-10%) of requiring a second minor outpatient operation.
“What we would expect is that by being more diligent in screening for and treating MEEs in these youngsters, we might get positive outcomes in speech and language development,” he added. “However, we need additional information on that.”